11/7/19
What is really happening to the children . . .
Sex trafficking is one topic that we learned about in class that really stood out to me as a major problem. We learned that there are many types of trafficking (sex, labor, intentional servitude, and child) along with the fact that many of these victims are part of the foster care system or have been a part of it. The reason for this can be attributed to the fact that the children who are put into the foster care system sometimes feel that no one cares about them and that they are not wanted. Thus, when a trafficker shows interest in them, they immediately take the opportunity to take this attention and what seems like love while it is being offered; however, the results never end up the way that these poor children had hoped. Many traffickers find their victims through social network, home neighborhoods, or clubs. The fact that social network is the primary way of finding victims really stood out to me since so many people are now using social media, especially starting at a younger age, too.
Although social media may be the leading cause of sex trafficking in developed countries, the reasons are quite different in developing countries. Child sex trafficking, specifically, is a very large problem. In Deanna Davy’s article “Understanding the complexities of responding to child sex trafficking in Thailand and Cambodia” (2014), she states the following: “Children, in contrast to adults, are clearly much more vulnerable and helpless against the established structures and vested interests in the sex sector, and are thus more likely to be victims of debt bondage, violence, exploitation or trafficking” (p. 794). These children do not really know what is going on when entering into these situations. The article continues to explain that some children see it necessary to enter into these affairs in order to help their family; whether it be to help with the family’s poverty or to fix some larger problem, they are just doing what they think has to be done (p. 794). It is quite sad that the children are under the impression that they need to turn themselves over to slavery in countries like Thailand and Cambodia in order to save their families. Children are not only turning themselves in but being turned over by their family members as well: “Some children are tuned over to recruiters by their families as part of an ancient practice known as debt bondage, in which children, usually girls, are sent to work for creditors until they pay off a family’s debt” (p. 794). This is the exact opposite of the situation in America and other developed countries. Instead of parents educating their children about trafficking and teaching them the warning signs on platforms where children are most susceptible, the parents are selling their children into the industry so that the family can stay on its feet and pay its debt.
As future healthcare providers, it is important that my peers and I know how to recognize signs of sex trafficking and violence. We need to be prepared to handle and care for patients who seem like they are victims of this industry. Specifically for when we travel to Guatemala this summer, we all should be on the lookout for children and women who are maybe being forced into the sex trade. Sex and child trafficking is a growing problem in developing countries, and more initiatives need to be taken to combat this problem.
Reference:
(2013) Retrieved from https://womennewsnetwork.net/2013/10/29/new-social-workers-cambodia/ .
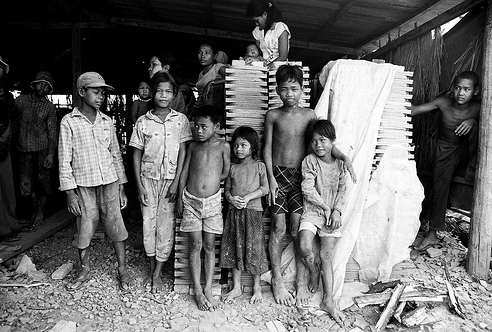
[Children in Cambodia] (2017). Retrieved from https://relevantmagazine.com/culture/global-culture/exposing-the-child-sex-trafficking-epidemic-in-cambodia/.
Davy, D. (2014). “Understanding the complexities of responding to child sex trafficking in Thailand and Cambodia.” International Journal of Sociology and Social Policy, 34(11), 793-816. https://www.emerald.com/insight/content/doi/10.1108/IJSSP-10-2013-0103/full/pdf?title=understanding-the-complexities-of-responding-to-child-sex-trafficking-in-thailand-and-cambodia.






